

54year-old male presents with back pain and know history of TB. IVP in the early excretory phase shows downward displacement of the lower pole calyces of the right kidney, non-filling of the upper calyces and a focal hypodense structure that appears to be displacing the lower pole calyces inferiorly. In addition there is significant loss of height of L3 with significant degenerative change at the L3-4 level
Ashley Davidoff MD TheCommonVein.net 115863
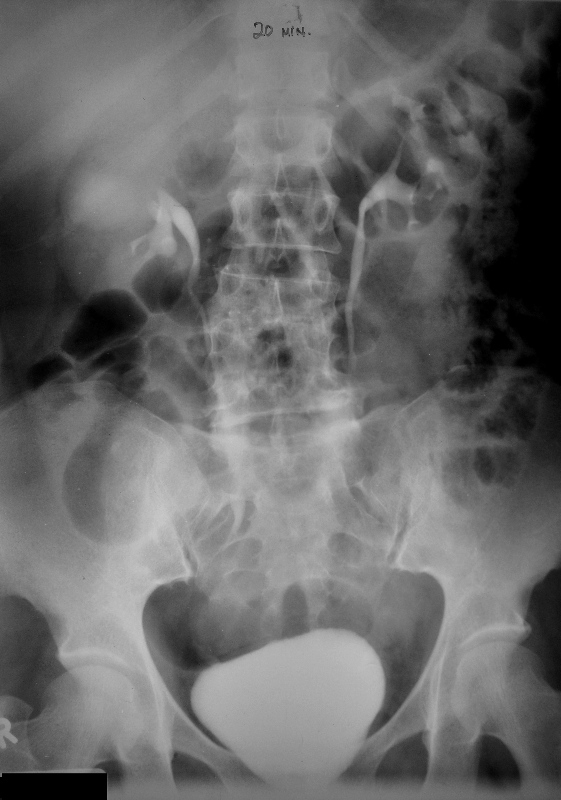
54year-old male presents with back pain and known history of TB. IVP in the late (20minute) excretory phase shows downward displacement of the lower pole calyces of the right kidney, and progressive -filling with contrast of the significantly hydronephrotic amorphous rotund middle calyces and suggestion of slow filling of minimally hydronephrotic upper pole calyces as a result of extrinsic compression from the severely dilated mid system. In addition, there is significant loss of height of L3 with significant degenerative change at the L3-4 level
These finding are consistent with TB of the kidney manifesting with infundibular stenosis of the mid calyces with primary severe obstruction in the middle calyces and secondary milder hydronephrosis of the upper pole calyces
Ashley Davidoff MD TheCommonVein.net 115866b

54year-old male presents with back pain and know history of TB. IVP in the late (20minute) excretory phase shows downward displacement of the lower pole calyces of the right kidney, and progressive -filling with contrast of the significantly hydronephrotic amorphous rotund middle calyces and suggestion of slow filling of minimally hydronephrotic upper pole calyces as a result of extrinsic compression from the severely dilated mid system. In addition, there is significant loss of height of L3 with significant degenerative change at the L3-4 level
These finding are consistent with TB of the kidney manifesting with infundibular stenosis of the mid calyces with primary severe obstruction in the middle calyces and secondary milder hydronephrosis of the upper pole calyces
Ashley Davidoff MD TheCommonVein.net 115868b

Axial CT through the upper abdomen shows a small shrunken left kidney with extensive corticomedullary calcification. The patient has a history of TB. The findings are consistent with autonephrectomy from TB of the kidney
Ashley Davidoff MD TheCommonVein.net 115859

58-year-old male with known history of tuberculosis. The CXR is normal with no active nor evidence of chronic granulomatous disease
The X ray of the lumbar spine shows a compression injury of the L1 vertebral body with compression of the superior endplate
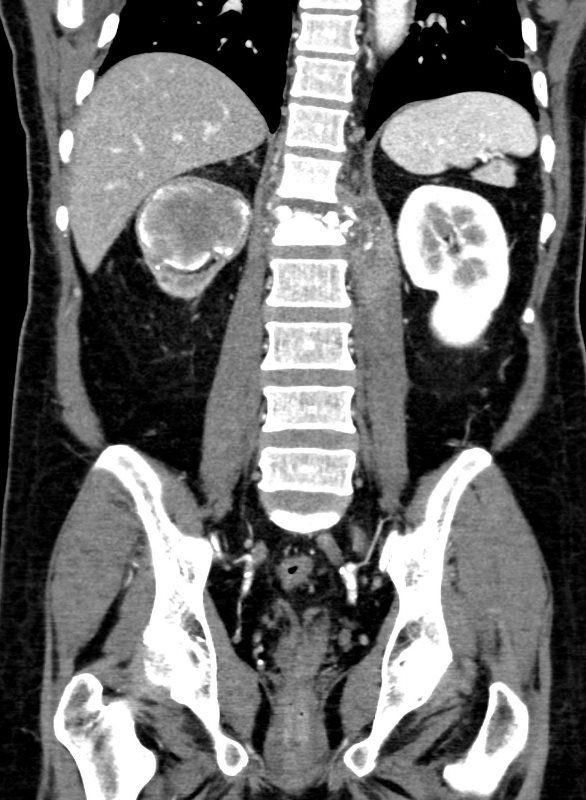
CT of the kidney shows replacement of the upper pole of the right kidney with focal hydronephrosis caused by infundibular stenosis and atrophy of the remainder of the right kidney.
There is enlargement of the bilateral adrenal glands, with multiple nodular structures encompassing the left adrenal gland, which may also represent infectious process.
Examination of the lumbar spine on the CT scan shows findings consistent with TB osteomyelitis with destruction of T12 and L1 vertebral bodies with prevertebral and epidural collections extending into the spinal canal.
The left psoas muscle shows peripherally enhancing communicating retroperitoneal and epidural fluid collection as well as multiple peripherally enhancing left psoas fluid collections.
Aspiration of the psoas muscle was performed
The MRI confirms the presence of an osteomyelitis discitis associated with an epidural abscess with multiple collections in the left psoas muscle
Contributed by Christina LeBedis MD
58-year-old male with known history of tuberculosis. The CXR is normal with no active nor evidence of chronic granulomatous disease
The X ray of the lumbar spine shows a compression injury of the L1 vertebral body with compression of the superior endplate
CT of the kidney shows replacement of the upper pole of the right kidney with focal hydronephrosis caused by infundibular stenosis and atrophy of the remainder of the right kidney.
There is enlargement of the bilateral adrenal glands, with multiple nodular structures encompassing the left adrenal gland, which may also represent infectious process.
Examination of the lumbar spine on the CT scan shows findings consistent with TB osteomyelitis with destruction of T12 and L1 vertebral bodies with prevertebral and epidural collections extending into the spinal canal.
The left psoas muscle shows peripherally enhancing communicating retroperitoneal and epidural fluid collection as well as multiple peripherally enhancing left psoas fluid collections.
Aspiration of the psoas muscle was performed
The MRI confirms the presence of an osteomyelitis discitis associated with an epidural abscess with multiple collections in the left psoas muscle
Contributed by Christina LeBedis MD

58-year-old male with known history of tuberculosis. The CXR is normal with no active nor evidence of chronic granulomatous disease
The X ray of the lumbar spine shows a compression injury of the L1 vertebral body with compression of the superior endplate
CT of the kidney shows replacement of the upper pole of the right kidney with focal hydronephrosis caused by infundibular stenosis and atrophy of the remainder of the right kidney.
There is enlargement of the bilateral adrenal glands, with multiple nodular structures encompassing the left adrenal gland, which may also represent infectious process.
Examination of the lumbar spine on the CT scan shows findings consistent with TB osteomyelitis with destruction of T12 and L1 vertebral bodies with prevertebral and epidural collections extending into the spinal canal.
The left psoas muscle shows peripherally enhancing communicating retroperitoneal and epidural fluid collection as well as multiple peripherally enhancing left psoas fluid collections.
Aspiration of the psoas muscle was performed
The MRI confirms the presence of an osteomyelitis discitis associated with an epidural abscess with multiple collections in the left psoas muscle
Contributed by Christina LeBedis MD